



















 Jan 27, 2020, 9:09 am
Jan 27, 2020, 9:09 am
Last edit by: username
PLEASE READ BEFORE POSTING
The following two links are updated daily:
IATA international transit / arrival policies Coronavirus Outbreak - Update
WHO Coronavirus disease (COVID-19) situation reports
Counters / Meters : Other Discussions on FlyerTalk Pertaining to COVID-19:
General (in this forum)
Location-specific
Airlines
Hotels
Other
Please add other discussions on FlyerTalk pertaining to COVID-19 not already been included in this WikiPost. Thank you.
This thread has become a valuable resource on Corona Virus/COVID-19 in general and no longer just about its impact on China travel. In order for the thread to remain fact-based and useful, posters are reminded to keep it free of speculation, conjecture and fear-mongering. Posts which do not meet these guidelines or which break the FT rules may be edited or deleted. Please observe the following FT rules in particular:
- be respectful and helpful
- stay on topic
- posts must be contributive to the thread
- inflammatory, inciting or unnecessarily provocative posts are not allowed
- repetitively posting comments of the same general theme is not permitted
- abusive, hateful, threatening, harassing or otherwise offensive posts will not be tolerated
- do not post comments on moderator decisions
FlyerTalk Senior Moderator Team
- be respectful and helpful
- stay on topic
- posts must be contributive to the thread
- inflammatory, inciting or unnecessarily provocative posts are not allowed
- repetitively posting comments of the same general theme is not permitted
- abusive, hateful, threatening, harassing or otherwise offensive posts will not be tolerated
- do not post comments on moderator decisions
FlyerTalk Senior Moderator Team
The following two links are updated daily:
IATA international transit / arrival policies Coronavirus Outbreak - Update
WHO Coronavirus disease (COVID-19) situation reports
Counters / Meters : Other Discussions on FlyerTalk Pertaining to COVID-19:
General (in this forum)
- Corona Virus / COVID-19 : general fact-based reporting [previously in] China forum
- COVID-19: Lounge thread for thoughts, concerns and questions
- USA halts entry of visitors who�ve been in UK, Ireland, Schengen countries
Location-specific
Airlines
- coronavirus travel waiver Air Canada | Aeroplan forum
- Coronavirus - Air China offers full refunds Other Asian, Australian, and South Pacific Airlines
- Does AFKL suspend flights to Mainland China? Air France, KLM, and Other Partners | Flying Blue
- NZ Suspends PVG service - till 29 March Air New Zealand | Air Points
- Alaska disappointing handling over an award ticket regarding viral outbreak in china Alaska Airlines | Mileage Plan
- AA China Coronavirus paid & award flights cancellation / change questions American Airlines | AAdvantage
- Coronavirus + NH All Nippon Airways | ANA Mileage Club
- *Coronavirus : BA Suspends all flts to mainland China* +discussion on long haul flts British Airways | Executive Club forum
- Wuhan coronavirus - effect on Cathay Pacific Cathay Pacific | Marco Polo Club
- China Southern travel-waiver corona-virus Other Asian, Australian, and South Pacific Airlines
- DL Coronavirus Waiver // Suspension of China flights due to Corona Virus Delta Air Lines / SkyMiles
- Coronavirus - Emirates Emirates | Skywards
- BR Adjusts Service/Schedule Due to Coronavirus Outbreak Eva Air / Infinity MileageLands
- Finnair China travel waivers?? Finnair | Finnair Plus
- Hainan Airlines (HU) Travel Waiver for 2019-nCoV? Other Asian, Australian, and South Pacific Airlines
- IB halts flights to China due to CoronaVirus [29/01/2020] Iberia Airlines | Iberia Plus
- Wuhan Coronavirus travel waiver / service change Japan Airlines | JAL Mileage Bank
- Coronavirus: LH Group general waiver to rebook flights operated end of April 2020 Lufthansa, Austrian, Swiss, Brussels, LOT and Other Partners | Miles & More
- Coronavirus: LH Group suspends flights to Italy [Discussion of Italy waiver] Lufthansa, Austrian, Swiss, Brussels, LOT and Other Partners | Miles & More
- Coronavirus Ticket Change Policy? Malaysia Airlines | Enrich
- QANTAS suspends services to China from Feb 9 Qantas | Frequent Flyer
- Ryanair - any options for Italy flights? Ryanair / Other European airlines
- SAS stops all direct flights to mainland China SAS | EuroBonus
- Coronavirus waivers Singapore Airlines | KrisFlyer
- THAI reduces flights to/from Mainland China 08Feb - 28Mar Thai Airways | Royal Orchid Plus
- Turkish Airlines Suspends Service to China until February 09 Turkish Airlines | Miles&Smiles
- UA COVID19: Flight Suspensions; Reduced serviced; Waivers; and No change fee bookings United Airlines | MileagePlus
- Coronavirus Waivers? Virgin Atlantic Airways | Flying Club
Hotels
- Cancellation of Bookings Due to Corona Virus Accor / ALL (Accor Live Limitless)
- Does Hilton wave no refundable bookings? Hilton / Hilton Honors
- CoronaVirus Cancellation - Non Refundable RESULT InterContinental Hotels / IHG Reward Club & Intercontinental Ambassador
- Coronavirus, any impact on your travel plan Marriott / Marriott Bonvoy
Other
- Which longhaul routes to/from China will be cut by end of Q1 2020? TravelBuzz
- Coronavirus epidemic, worries for China/ Global GDP OmniPR forum
- Coronavirus in the US. What would Amtrak do? Amtrak / Guest Rewards
- Your Next Cruise: Are are Having Second Thoughts Due to Fears of Pandemic? Travel&Dining / Cruises
Please add other discussions on FlyerTalk pertaining to COVID-19 not already been included in this WikiPost. Thank you.

Coronavirus / COVID-19 : general fact-based reporting
Mar 1, 2021, 1:28 pm
#7591
Suspended
Join Date: Feb 2009
Programs: DL, UA, AA, VS
Posts: 5,226
Not surprising, the top super-spreader venues:
 Mar 2, 2021, 12:22 am
Mar 2, 2021, 12:22 am
#7592
Join Date: Sep 2015
Location: Between Seas
Posts: 4,754
Anecdotally, Pfizer has milder side effects compared to AZ on the first dose, but it <switches> around for the second dose, so Pfizer is a bit tougher on the second dose whereas side effects are lower for AZ's second dose. Moderna we don't have yet. More of a nuisance than a problem, overall, many people barely notice anything. On the other hand anecdotally some people report improvements to unrelated long term conditions shortly after vaccination. This isn't unusual, the polio vaccine also had some extra benefits beyond polio itself. So in the round it shouldn't deter anyone getting the vaccine.
It may be that 50% trial success against mild infections and 80% against severe or worse with Sinovac type is still better than near 0% without any, from a general public-health viewpoint. Personally, I see it best to go for the 90+% immunity induced by Pfizer or Moderna mRNA vaccines, where indicated and available soonest.
Last edited by FlitBen; Mar 2, 2021 at 1:20 am
Mar 2, 2021, 1:55 am
#7593
Moderator, Iberia Airlines, Airport Lounges, and Ambassador, British Airways Executive Club
Join Date: Feb 2010
Programs: BA Lifetime Gold; Flying Blue Life Platinum; LH Sen.; Hilton Diamond; Kemal Kebabs Prized Customer
Posts: 63,850
Upthread I put a link to the Public Health Scotland / Edinburgh University real world pre-print of 1.14 million residents of Scotland who have received either the Pfizer or AstraZeneca vaccine. The results were much better than the clinical trial results. And I will make another reference to REACT-2, also linked above.
Here is the pre-print of the English version, including the results from 7.6 million residents in England on the same vaccines. The rollout in the UK was skewed towards vaccinating the most vulnerable citizens first. This is led by Public Health England and the London School of Hygiene and Tropical Medicine. As with Scotland these are early figures since it's only been since early January that the UK numbers vaccinated started to pick up, which then takes you to early February to start seeing anything interesting. But the headlines are for those over 70 years of age
- 60% to 89% protection against symptomatic disease
- 80% plus protection against severe disease requiring hospitalisation
- 83% plus protection against death
To illustrate that, someone in the late 80s or early 90s who has been vaccinated will have a near equal or better chance of surviving the worst effects of Covid compared to someone in their mid 50s. We don't have the data for the impacts on younger people yet, but I would obviously expect that to be an even better outcome. The report didn't look into transmission but we've seen elsewhere that is demonstrated with UK healthworkers.
As with Scotland there is some evidence that AstraZeneca is marginally more effective than Pfizer, particularly over time, however there are fewer case studies to look at since Pfizer was rolled out before AZ.
https://khub.net/documents/135939561...=1614617945615
Here is the pre-print of the English version, including the results from 7.6 million residents in England on the same vaccines. The rollout in the UK was skewed towards vaccinating the most vulnerable citizens first. This is led by Public Health England and the London School of Hygiene and Tropical Medicine. As with Scotland these are early figures since it's only been since early January that the UK numbers vaccinated started to pick up, which then takes you to early February to start seeing anything interesting. But the headlines are for those over 70 years of age
- 60% to 89% protection against symptomatic disease
- 80% plus protection against severe disease requiring hospitalisation
- 83% plus protection against death
To illustrate that, someone in the late 80s or early 90s who has been vaccinated will have a near equal or better chance of surviving the worst effects of Covid compared to someone in their mid 50s. We don't have the data for the impacts on younger people yet, but I would obviously expect that to be an even better outcome. The report didn't look into transmission but we've seen elsewhere that is demonstrated with UK healthworkers.
As with Scotland there is some evidence that AstraZeneca is marginally more effective than Pfizer, particularly over time, however there are fewer case studies to look at since Pfizer was rolled out before AZ.
https://khub.net/documents/135939561...=1614617945615
Mar 2, 2021, 5:24 am
#7594
Join Date: Oct 2004
Location: Greater Chicagoland Area
Programs: frontier Elite, Hertz PC
Posts: 1,455
https://www.nbcchicago.com/news/coro...k/2450706/?amp
Johnson & Johnson vaccine shipments began Monday and already, Chicago and Illinois are preparing for an estimated dose count above 100,000 this week.
Mar 2, 2021, 5:25 am
#7595


Join Date: Nov 2012
Location: Rhineland-Palatinate
Programs: *A Gold (A3), HHonor Gold
Posts: 5,701
JAMA did a great piece about all current vaccines for COVID-19, with a handy summary table:
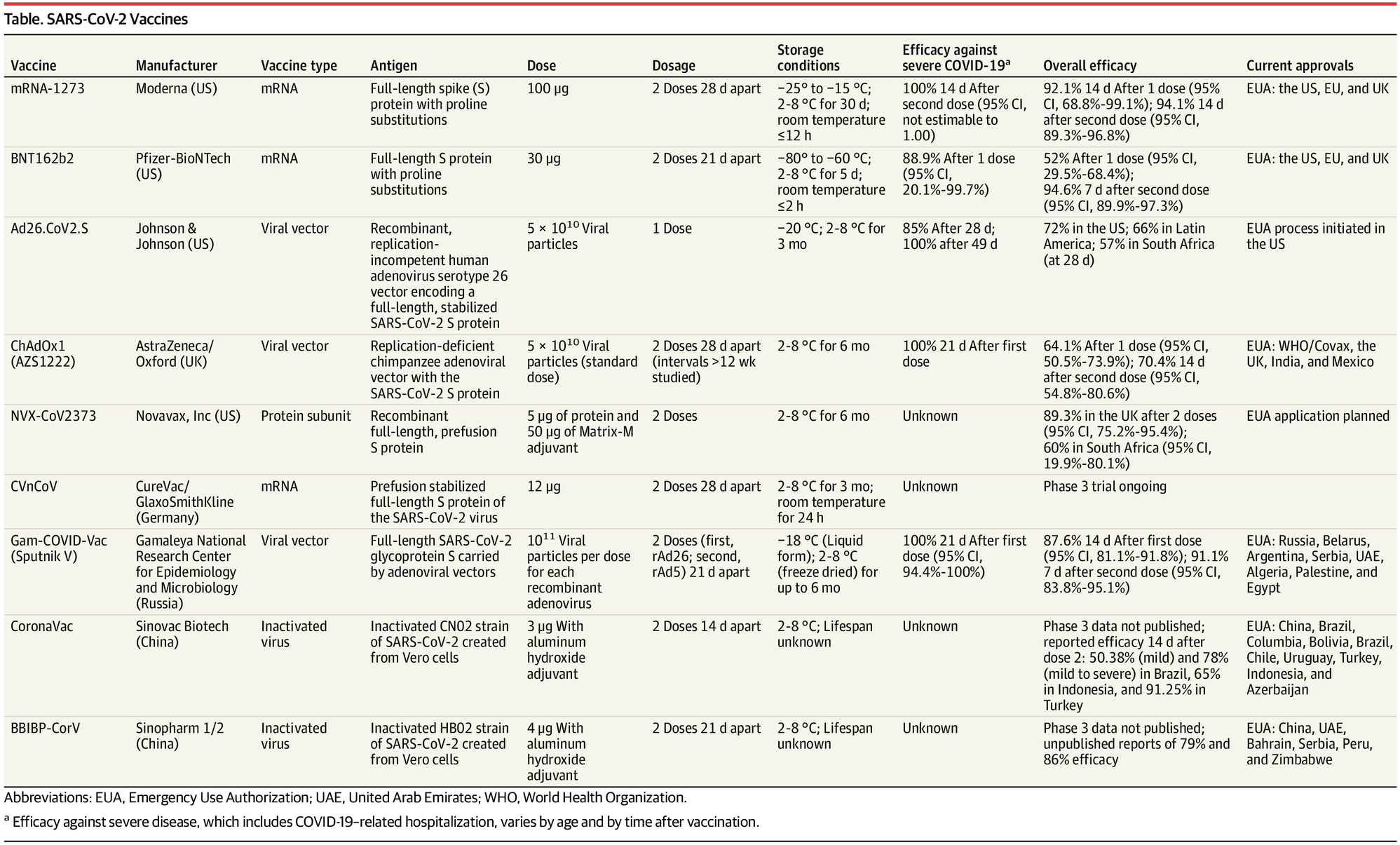
https://jamanetwork.com/journals/jam...rticle/2777059
And here is an interesting study from Germany about risk of aerosol transmission in various locals and settings (occupation, masks). School is at the top of the list, even masked, due to high density and typical lack of aeration of schools (in a couple of countries it is forbidden to open school windows if at ground floor due to anti terrorist regulations)
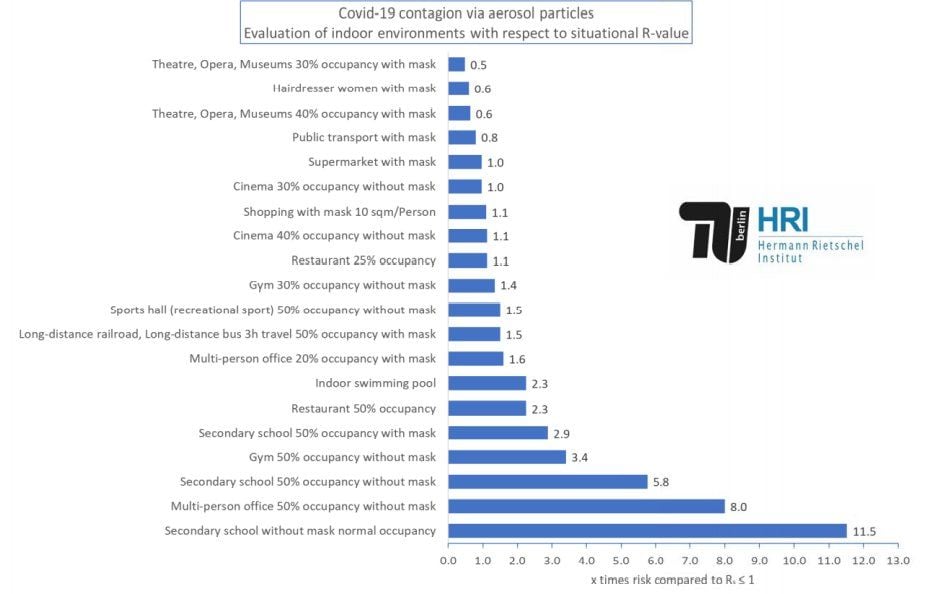
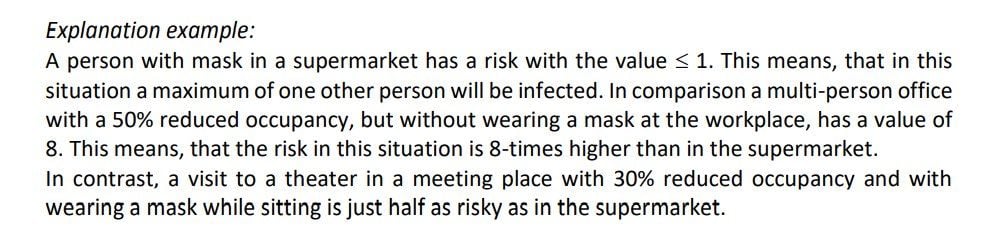
https://depositonce.tu-berlin.de/handle/11303/12578
Vaccination is the most important strategy to end the pandemic. However, emergence of multiple SARS-CoV-2 variants with reduced susceptibility to disease- and vaccine-induced immunity threatens progress. Despite these ongoing threats, the efficacy of SARS-CoV-2 vaccines provides a real measure of hope for 2021.
And here is an interesting study from Germany about risk of aerosol transmission in various locals and settings (occupation, masks). School is at the top of the list, even masked, due to high density and typical lack of aeration of schools (in a couple of countries it is forbidden to open school windows if at ground floor due to anti terrorist regulations)
https://depositonce.tu-berlin.de/handle/11303/12578
Mar 2, 2021, 9:28 am
#7596
Join Date: Jan 2019
Programs: UA
Posts: 42
As with Scotland there is some evidence that AstraZeneca is marginally more effective than Pfizer, particularly over time, however there are fewer case studies to look at since Pfizer was rolled out before AZ.
https://khub.net/documents/135939561...=1614617945615
https://khub.net/documents/135939561...=1614617945615
Below is the actual quote from the article, with my emphasis added.
"We find that a single dose of the BNT162b2 vaccine is approximately 60-70% effective at preventing symptomatic disease in adults aged 70 years and older in England and 2 doses are approximately 85-90% effective. Those vaccinated who went on to become a symptomatic case had a 44% lower risk of hospitalisation and a 51% lower risk of death compared to unvaccinated cases. We also provide the first real world evidence of effectiveness of the ChAdOx1 vaccine. The effect of a single dose of the ChAdOx1 vaccine against symptomatic disease was approximately 60-75%"
So, AZ after one dose seems to do roughly as well as Pfizer after one dose ("60-70%" vs. "60-75%"). Not better...about the same. But that's arguably not the appropriate comparison because Pfizer's vaccine is intended to be administered twice. After the second dose, it's "85-90%" effective, which is clearly better than AZ's 60-75% efficacy.
The Scotland article goes on to note that other studies have now shown that the Pfizer vaccine is about 90% effective after the second dose, including the original clinical trial and the Israeli study. There's also a U.S. study (not yet peer reviewed) that reported about 88% efficacy in the real world. https://www.medrxiv.org/content/10.1....15.21251623v1
If you really want to advocate for AZ, you could argue that it's cheaper and more convenient (one vs. two shots). You could also argue that AZ might have been just as effective if only you could get two doses of it. But that's not an option, so far as I know, and there appear to be little data supporting that conjecture. The original Voysey study had a two-dose condition that showed only 62�1% efficacy (95% CI 41�75%). That's well below the efficacy found in all of the Pfizer two-dose studies. The AZ clinical trial did find better results for a half dose followed by a regular dose. https://www.thelancet.com/action/sho...2820%2932661-1 Maybe they should have followed up on that. But the error bars were quite wide (95% CI 75-95%) and I don't know that it has been replicated and I don't recall that dosing regimen actually being adopted in practice.
Mar 2, 2021, 9:57 am
#7597
Moderator, Iberia Airlines, Airport Lounges, and Ambassador, British Airways Executive Club
Join Date: Feb 2010
Programs: BA Lifetime Gold; Flying Blue Life Platinum; LH Sen.; Hilton Diamond; Kemal Kebabs Prized Customer
Posts: 63,850
The AZ r�gime is for two doses too, it should be pointed out. The National Protocol remains two doses between 4 and 12 weeks apart. The point I was making was that in the margins some of the data for AZ was slightly better - the 94% for AZ in the PHS table for example. I am not making a big claim here, this comment was obviously more directed at those who felt that AZ was quasi-ineffective for the elderly and were perhaps waiting to get Pfizer - and this would be a mistake. Both vaccines do a great job, and people should get either of them at the first opportunity.
Mar 2, 2021, 11:06 am
#7598
FlyerTalk Evangelist
Join Date: Nov 2004
Location: 45� North
Programs: DL DM MM, HH Diamond
Posts: 10,196
Here is the pre-print of the English version, including the results from 7.6 million residents in England on the same vaccines. The rollout in the UK was skewed towards vaccinating the most vulnerable citizens first. This is led by Public Health England and the London School of Hygiene and Tropical Medicine. As with Scotland these are early figures since it's only been since early January that the UK numbers vaccinated started to pick up, which then takes you to early February to start seeing anything interesting. But the headlines are for those over 70 years of age
- 60% to 89% protection against symptomatic disease
- 80% plus protection against severe disease requiring hospitalisation
- 83% plus protection against death
- 60% to 89% protection against symptomatic disease
- 80% plus protection against severe disease requiring hospitalisation
- 83% plus protection against death
Mar 2, 2021, 11:29 am
#7599
Moderator, Iberia Airlines, Airport Lounges, and Ambassador, British Airways Executive Club
Join Date: Feb 2010
Programs: BA Lifetime Gold; Flying Blue Life Platinum; LH Sen.; Hilton Diamond; Kemal Kebabs Prized Customer
Posts: 63,850
Yes, good point, it's against those who don't get any vaccine at all. It demonstrates the velue of having a vaccine at all, in mass roll-out terms, given that the clinical trial data has some limitations on it.
Mar 2, 2021, 1:25 pm
#7600
Join Date: Mar 2009
Location: LAX
Posts: 3,267
The strongest protection might actually come from mixing vaccines, rather than sticking with one type.
https://www.latimes.com/science/stor...id-19-vaccines
This month, a team of vaccinologists from Oxford University began recruiting 800 or so people age 50 or older for a complex study to see whether vaccine switching could actually work.Using an eight-armed clinical trial, they’ll test vaccine regimens using various combinations and intervals of the two vaccines currently being dispensed in Britain: one made by Pfizer and BioNTech, and another developed by Oxford and AstraZeneca.
In announcing the mix-and-match vaccine trial, Dr. Matthew Snape cited experiments in mice in which combinations of the Pfizer and AstraZeneca vaccines boosted immunity better than two doses of either one alone. Perhaps it would work in humans as well.
Both vaccines prime the immune system to target the coronavirus’ spike protein, which plays an instrumental role in the infection process. But they home in on different parts of the spike, and they deliver their payloads by two very different means.
In announcing the mix-and-match vaccine trial, Dr. Matthew Snape cited experiments in mice in which combinations of the Pfizer and AstraZeneca vaccines boosted immunity better than two doses of either one alone. Perhaps it would work in humans as well.
Both vaccines prime the immune system to target the coronavirus’ spike protein, which plays an instrumental role in the infection process. But they home in on different parts of the spike, and they deliver their payloads by two very different means.
Mar 3, 2021, 1:18 am
#7601
Join Date: Jun 2019
Posts: 281
Is there anything wrong with someone who had corona to get 2 doses? Is there such a thing as not healthy to have too many antibodies? E.G. if someone wants to get both the Pfizer and AZ to maximize protection, anything wrong?
I know someone in their 90's that got 2 Pfizer doses and still got negative antibody tests. So could they get the AZ too see if that helps?
I know someone in their 90's that got 2 Pfizer doses and still got negative antibody tests. So could they get the AZ too see if that helps?
Mar 3, 2021, 6:25 am
#7602
Join Date: Sep 2015
Location: Between Seas
Posts: 4,754
Is there anything wrong with someone who had corona to get 2 doses? Is there such a thing as not healthy to have too many antibodies? E.G. if someone wants to get both the Pfizer and AZ to maximize protection, anything wrong?
I know someone in their 90's that got 2 Pfizer doses and still got negative antibody tests. So could they get the AZ too see if that helps?
I know someone in their 90's that got 2 Pfizer doses and still got negative antibody tests. So could they get the AZ too see if that helps?
Millions of AstraZeneca shots 'ineffective' if South Africa variant in PH not contained, expert warns
- OCTA Research fellow and molecular biologist Fr. Nicanor Austriaco quoted several studies showing that the South Africa variant lowers the efficacy of some COVID-19 vaccines. He specifically stated the vaccines made by British-Swedish multinational pharmaceutical Oxford-AstraZeneca, saying the variant dramatically decreases the vaccine's efficacy from 70% to mere 10%. "It's no different than injecting water into the patients. With 10% protection, basically, most people would still get mild and moderate COVID-19," he said in a media briefing.
The Philippines is set to receive its second batch of vaccines on Thursday — 487,200 doses of AstraZeneca through the COVAX facility. This is on top of more than 17 million doses procured by the government and private firms through tripartite agreements. Austriaco, who is developing an oral COVID-19 vaccine in the United States, said the presence of the South Africa variant could also affect the rollout of the national vaccination program if the spread is not cut off. –
- OCTA Research fellow and molecular biologist Fr. Nicanor Austriaco quoted several studies showing that the South Africa variant lowers the efficacy of some COVID-19 vaccines. He specifically stated the vaccines made by British-Swedish multinational pharmaceutical Oxford-AstraZeneca, saying the variant dramatically decreases the vaccine's efficacy from 70% to mere 10%. "It's no different than injecting water into the patients. With 10% protection, basically, most people would still get mild and moderate COVID-19," he said in a media briefing.
The Philippines is set to receive its second batch of vaccines on Thursday — 487,200 doses of AstraZeneca through the COVAX facility. This is on top of more than 17 million doses procured by the government and private firms through tripartite agreements. Austriaco, who is developing an oral COVID-19 vaccine in the United States, said the presence of the South Africa variant could also affect the rollout of the national vaccination program if the spread is not cut off. –
Mar 3, 2021, 6:48 am
#7603
Join Date: Nov 2012
Location: Rhineland-Palatinate
Programs: *A Gold (A3), HHonor Gold
Posts: 5,701
A Swedish researcher, who signed the Great Barrington Declaration and whose research was key in keeping school open actually had eliminated key data that were contradicting his pre-determined conclusion that school should stay open.
https://www.sciencemag.org/news/2021...-risks-swedish
Pediatrician and epidemiologist Jonas Ludvigsson of Sweden’s Karolinska Institute has been a staunch defender of his country’s unorthodox coronavirus policies. Among them was the decision in the spring of 2020 to keep preschools and schools open for children through grade nine, despite limited understanding of the virus and with few precautions to prevent school outbreaks. But Ludvigsson’s research, which suggested that policy was relatively safe—and has been widely cited in arguments against school closures—has repeatedly come under fire from critics of Sweden’s approach.
The latest example is a research letter, published online by The New England Journal of Medicine (NEJM) on 6 January, that looked at severe disease and deaths among children and teachers in Sweden between March and June 2020. Critics—including the authors of two letters NEJM published on 1 March—have said the study was beside the point and a distraction. It’s well known that children are less likely to be hospitalized or die from COVID-19; instead, schools worldwide have shut down to slow the spread of the virus in the wider community.
But Science has learned that another complaint sent to NEJM makes a more serious allegation: that the authors deliberately left out key data that contradicted their conclusion.The complaint comes from Bodil Malmberg, a private citizen in V�rg�rda, Sweden. She used the country’s open records law to obtain email correspondence between Ludvigsson and Swedish chief epidemiologist Anders Tegnell, the architect of the country’s pandemic policies, that shed light on how the paper came about. Malmberg says she requested the emails because the data in the NEJM paper “did not add up.” Ludvigsson does not dispute the content of the emails, but stands by the study’s conclusions. However, he says the barrage of criticism and personal attacks has made him decide to quit COVID-19 research.
Ludvigsson, whose prepandemic research focused on gastroenterology, was one of the 47 original signers of the Great Barrington Declaration, a controversial document published in October 2020 that argued that pandemic policies should focus on protecting the vulnerable while the rest of the population builds up immunity through natural infection.
Ludvigsson’s research seemed to support those ideas. In a review about children’s role in the pandemic, published in Acta Paediatrica in May 2020, he reported there had been “no major school outbreaks in Sweden,” which he attributed to “personal communication” from Tegnell. But as critics noted, Swedish media had reported several school outbreaks by then, including one in which at least 18 of 76 staff were infected and one teacher died. (Children were not tested.)
His NEJM letter sounded another reassuring note. It reported that in all of Sweden, only 15 children, 10 preschool teachers, and 20 school teachers were admitted to intensive care units for COVID-19 complications between March and June 2020. The authors noted that 69 children ages 1 to 16 died of any cause in Sweden during that same period, compared with 65 between November 2019 and February 2020, suggesting the pandemic had not led to an increase in child deaths.
But the emails obtained by Malmberg show that in July 2020, Ludvigsson wrote to Tegnell that “unfortunately we see a clear indication of excess mortality among children ages 7-16 old, the ages where ‘kids went to school.’” For the years 2015 through 2019, an average of 30.4 children in that age group died in the four spring months; in 2020, 51 children in that age group died, “= excess mortality +68%,” Ludvigsson wrote. The increase could be a fluke, he wrote, especially because the numbers are small. Deaths in 1- to 6-year-olds were below average during the same period, so combining the age groups helped even out the increase, he noted.
The emails “cast a serious shadow” on the research letter, Malmberg wrote in an email to NEJM. (The journal declined to comment on her complaint.) Epidemiologist Jonas Bj�rk of Lund University agrees that the time comparison used in the paper was unusual. “I can see no good reason to compare with previous months,” he says. “It is standard to compare with the same period in previous years” to account for seasonality and to decrease statistical uncertainty.
The latest example is a research letter, published online by The New England Journal of Medicine (NEJM) on 6 January, that looked at severe disease and deaths among children and teachers in Sweden between March and June 2020. Critics—including the authors of two letters NEJM published on 1 March—have said the study was beside the point and a distraction. It’s well known that children are less likely to be hospitalized or die from COVID-19; instead, schools worldwide have shut down to slow the spread of the virus in the wider community.
But Science has learned that another complaint sent to NEJM makes a more serious allegation: that the authors deliberately left out key data that contradicted their conclusion.The complaint comes from Bodil Malmberg, a private citizen in V�rg�rda, Sweden. She used the country’s open records law to obtain email correspondence between Ludvigsson and Swedish chief epidemiologist Anders Tegnell, the architect of the country’s pandemic policies, that shed light on how the paper came about. Malmberg says she requested the emails because the data in the NEJM paper “did not add up.” Ludvigsson does not dispute the content of the emails, but stands by the study’s conclusions. However, he says the barrage of criticism and personal attacks has made him decide to quit COVID-19 research.
Ludvigsson, whose prepandemic research focused on gastroenterology, was one of the 47 original signers of the Great Barrington Declaration, a controversial document published in October 2020 that argued that pandemic policies should focus on protecting the vulnerable while the rest of the population builds up immunity through natural infection.
Ludvigsson’s research seemed to support those ideas. In a review about children’s role in the pandemic, published in Acta Paediatrica in May 2020, he reported there had been “no major school outbreaks in Sweden,” which he attributed to “personal communication” from Tegnell. But as critics noted, Swedish media had reported several school outbreaks by then, including one in which at least 18 of 76 staff were infected and one teacher died. (Children were not tested.)
His NEJM letter sounded another reassuring note. It reported that in all of Sweden, only 15 children, 10 preschool teachers, and 20 school teachers were admitted to intensive care units for COVID-19 complications between March and June 2020. The authors noted that 69 children ages 1 to 16 died of any cause in Sweden during that same period, compared with 65 between November 2019 and February 2020, suggesting the pandemic had not led to an increase in child deaths.
But the emails obtained by Malmberg show that in July 2020, Ludvigsson wrote to Tegnell that “unfortunately we see a clear indication of excess mortality among children ages 7-16 old, the ages where ‘kids went to school.’” For the years 2015 through 2019, an average of 30.4 children in that age group died in the four spring months; in 2020, 51 children in that age group died, “= excess mortality +68%,” Ludvigsson wrote. The increase could be a fluke, he wrote, especially because the numbers are small. Deaths in 1- to 6-year-olds were below average during the same period, so combining the age groups helped even out the increase, he noted.
The emails “cast a serious shadow” on the research letter, Malmberg wrote in an email to NEJM. (The journal declined to comment on her complaint.) Epidemiologist Jonas Bj�rk of Lund University agrees that the time comparison used in the paper was unusual. “I can see no good reason to compare with previous months,” he says. “It is standard to compare with the same period in previous years” to account for seasonality and to decrease statistical uncertainty.
Mar 3, 2021, 7:14 am
#7604
FlyerTalk Evangelist
Join Date: Nov 2004
Location: 45� North
Programs: DL DM MM, HH Diamond
Posts: 10,196
To note: this is a way some researchers can tell if a vaccinated person has also been infected. If they have ABs to N and S they may have been infected with SARS-CoV-2.
Mar 3, 2021, 8:18 am
#7605
Moderator, Iberia Airlines, Airport Lounges, and Ambassador, British Airways Executive Club
Join Date: Feb 2010
Programs: BA Lifetime Gold; Flying Blue Life Platinum; LH Sen.; Hilton Diamond; Kemal Kebabs Prized Customer
Posts: 63,850
Is there anything wrong with someone who had corona to get 2 doses? Is there such a thing as not healthy to have too many antibodies? E.G. if someone wants to get both the Pfizer and AZ to maximize protection, anything wrong?
I know someone in their 90's that got 2 Pfizer doses and still got negative antibody tests. So could they get the AZ too see if that helps?
I know someone in their 90's that got 2 Pfizer doses and still got negative antibody tests. So could they get the AZ too see if that helps?
Originally Posted by Public Health England - National protocol for COVID-19 Vaccine AstraZeneca - ChAdOx1-S (recombinant)
Vaccination of individuals who may be infected but asymptomatic or incubating COVID-19 infection is unlikely to have a detrimental effect on the illness. Vaccination should be deferred in those with confirmed infection to avoid onward transmission and confusing the differential diagnosis. As clinical deterioration can occur up to two weeks after infection, ideally vaccination should be deferred until clinical recovery to around four weeks after onset of symptoms or four weeks from the first confirmed positive specimen in those who are asymptomatic.
The idea of mixing vacccines is a bit wierd for those of us who go through vaccination data, since the vaccination effect is after the onslaught of the immunity complex. How you get that onslaught shouldn't matter much, it is what happens after that is interesting. Still, there are surveys and studies going on, and some of my customers are participating in field studies at the Newcastle RVI - I think I've now had every combination of J&J, Moderna, Novaavax, Pfizer and AZ. So in a few months we will soon find out if there is a magic pick-and-mix combo.
Negative antibody after vaccination doesn't mean no protection, you are just relying on T cells rather than B cells. In the UK we wouldn't be too concerned about someone in that position, but I must admit I would perhaps them down as an early candidate for the autumn 2021 booster, perhaps using a different technology. But no vaccine is 100% perfect, nor, actually, does it need to be.