



















 Jan 27, 2020, 9:09 am
Jan 27, 2020, 9:09 am
Last edit by: username
PLEASE READ BEFORE POSTING
The following two links are updated daily:
IATA international transit / arrival policies Coronavirus Outbreak - Update
WHO Coronavirus disease (COVID-19) situation reports
Counters / Meters : Other Discussions on FlyerTalk Pertaining to COVID-19:
General (in this forum)
Location-specific
Airlines
Hotels
Other
Please add other discussions on FlyerTalk pertaining to COVID-19 not already been included in this WikiPost. Thank you.
This thread has become a valuable resource on Corona Virus/COVID-19 in general and no longer just about its impact on China travel. In order for the thread to remain fact-based and useful, posters are reminded to keep it free of speculation, conjecture and fear-mongering. Posts which do not meet these guidelines or which break the FT rules may be edited or deleted. Please observe the following FT rules in particular:
- be respectful and helpful
- stay on topic
- posts must be contributive to the thread
- inflammatory, inciting or unnecessarily provocative posts are not allowed
- repetitively posting comments of the same general theme is not permitted
- abusive, hateful, threatening, harassing or otherwise offensive posts will not be tolerated
- do not post comments on moderator decisions
FlyerTalk Senior Moderator Team
- be respectful and helpful
- stay on topic
- posts must be contributive to the thread
- inflammatory, inciting or unnecessarily provocative posts are not allowed
- repetitively posting comments of the same general theme is not permitted
- abusive, hateful, threatening, harassing or otherwise offensive posts will not be tolerated
- do not post comments on moderator decisions
FlyerTalk Senior Moderator Team
The following two links are updated daily:
IATA international transit / arrival policies Coronavirus Outbreak - Update
WHO Coronavirus disease (COVID-19) situation reports
Counters / Meters : Other Discussions on FlyerTalk Pertaining to COVID-19:
General (in this forum)
- Corona Virus / COVID-19 : general fact-based reporting [previously in] China forum
- COVID-19: Lounge thread for thoughts, concerns and questions
- USA halts entry of visitors who�ve been in UK, Ireland, Schengen countries
Location-specific
Airlines
- coronavirus travel waiver Air Canada | Aeroplan forum
- Coronavirus - Air China offers full refunds Other Asian, Australian, and South Pacific Airlines
- Does AFKL suspend flights to Mainland China? Air France, KLM, and Other Partners | Flying Blue
- NZ Suspends PVG service - till 29 March Air New Zealand | Air Points
- Alaska disappointing handling over an award ticket regarding viral outbreak in china Alaska Airlines | Mileage Plan
- AA China Coronavirus paid & award flights cancellation / change questions American Airlines | AAdvantage
- Coronavirus + NH All Nippon Airways | ANA Mileage Club
- *Coronavirus : BA Suspends all flts to mainland China* +discussion on long haul flts British Airways | Executive Club forum
- Wuhan coronavirus - effect on Cathay Pacific Cathay Pacific | Marco Polo Club
- China Southern travel-waiver corona-virus Other Asian, Australian, and South Pacific Airlines
- DL Coronavirus Waiver // Suspension of China flights due to Corona Virus Delta Air Lines / SkyMiles
- Coronavirus - Emirates Emirates | Skywards
- BR Adjusts Service/Schedule Due to Coronavirus Outbreak Eva Air / Infinity MileageLands
- Finnair China travel waivers?? Finnair | Finnair Plus
- Hainan Airlines (HU) Travel Waiver for 2019-nCoV? Other Asian, Australian, and South Pacific Airlines
- IB halts flights to China due to CoronaVirus [29/01/2020] Iberia Airlines | Iberia Plus
- Wuhan Coronavirus travel waiver / service change Japan Airlines | JAL Mileage Bank
- Coronavirus: LH Group general waiver to rebook flights operated end of April 2020 Lufthansa, Austrian, Swiss, Brussels, LOT and Other Partners | Miles & More
- Coronavirus: LH Group suspends flights to Italy [Discussion of Italy waiver] Lufthansa, Austrian, Swiss, Brussels, LOT and Other Partners | Miles & More
- Coronavirus Ticket Change Policy? Malaysia Airlines | Enrich
- QANTAS suspends services to China from Feb 9 Qantas | Frequent Flyer
- Ryanair - any options for Italy flights? Ryanair / Other European airlines
- SAS stops all direct flights to mainland China SAS | EuroBonus
- Coronavirus waivers Singapore Airlines | KrisFlyer
- THAI reduces flights to/from Mainland China 08Feb - 28Mar Thai Airways | Royal Orchid Plus
- Turkish Airlines Suspends Service to China until February 09 Turkish Airlines | Miles&Smiles
- UA COVID19: Flight Suspensions; Reduced serviced; Waivers; and No change fee bookings United Airlines | MileagePlus
- Coronavirus Waivers? Virgin Atlantic Airways | Flying Club
Hotels
- Cancellation of Bookings Due to Corona Virus Accor / ALL (Accor Live Limitless)
- Does Hilton wave no refundable bookings? Hilton / Hilton Honors
- CoronaVirus Cancellation - Non Refundable RESULT InterContinental Hotels / IHG Reward Club & Intercontinental Ambassador
- Coronavirus, any impact on your travel plan Marriott / Marriott Bonvoy
Other
- Which longhaul routes to/from China will be cut by end of Q1 2020? TravelBuzz
- Coronavirus epidemic, worries for China/ Global GDP OmniPR forum
- Coronavirus in the US. What would Amtrak do? Amtrak / Guest Rewards
- Your Next Cruise: Are are Having Second Thoughts Due to Fears of Pandemic? Travel&Dining / Cruises
Please add other discussions on FlyerTalk pertaining to COVID-19 not already been included in this WikiPost. Thank you.

Coronavirus / COVID-19 : general fact-based reporting
May 30, 2020, 9:50 am
#5371
Join Date: Mar 2005
Programs: Continental Onepass, Hilton, Marriott, USAir and now UA
Posts: 6,440
New article from the WSJ on the origins of the Covid virus. Unfortunately behind a pay wall but someone may know a work around.
https://www.wsj.com/articles/so-wher...om-11590756909
The Lancet article on hydroxychloroquin gets a correction but no change in the author's conclusions.
While I referenced a Buzzfeed article on the correction, I do recommend looking at the original correction for which there is a link in the journalist's paper. I would not rely on Buzzfeed's analysis of anything as the final word.
https://www.buzzfeednews.com/article...-letter-lancet
As I wrote in an earlier commentary about the Lancet report, it was a registration study, not a randomized controlled study and therefore would suffer the defects inherent in any registration study, which includes investigator bias, inaccurate registration and imbalanced participation groupings, to name a few.
There are always dangers in relying on incomplete studies to make treatment decisions. If the POTUS had never mentioned the drug, no one would have cared about it, TBH.
.
https://www.wsj.com/articles/so-wher...om-11590756909
The Lancet article on hydroxychloroquin gets a correction but no change in the author's conclusions.
While I referenced a Buzzfeed article on the correction, I do recommend looking at the original correction for which there is a link in the journalist's paper. I would not rely on Buzzfeed's analysis of anything as the final word.
https://www.buzzfeednews.com/article...-letter-lancet
As I wrote in an earlier commentary about the Lancet report, it was a registration study, not a randomized controlled study and therefore would suffer the defects inherent in any registration study, which includes investigator bias, inaccurate registration and imbalanced participation groupings, to name a few.
There are always dangers in relying on incomplete studies to make treatment decisions. If the POTUS had never mentioned the drug, no one would have cared about it, TBH.
.
Last edited by NewbieRunner; May 31, 2020 at 10:27 am Reason: Merge consecutive posts by same member
 May 30, 2020, 11:05 am
May 30, 2020, 11:05 am
#5372
Suspended
Join Date: Oct 2004
Location: Bay Area
Programs: DL SM, UA MP.
Posts: 12,729
New article from the WSJ on the origins of the Covid virus. Unfortunately behind a pay wall but someone may know a work around.
https://www.wsj.com/articles/so-wher...om-11590756909
https://www.wsj.com/articles/so-wher...om-11590756909
May 30, 2020, 11:16 am
#5373
Join Date: Dec 2018
Location: PHX
Programs: Delta DM, Marriott Lifetime Titanium, HHonrs Diamond
Posts: 1,336
It is an opinion piece by a single author.
I read it and cannot find a free link, but here is the take home point....
I read it and cannot find a free link, but here is the take home point....
The closest animal version of the virus remains a bat sample collected by scientists in 2013 a thousand miles away in Yunnan. Details of where and how that sample was collected have been sketchy, but a new paper by two scientists from the Agharkar Research Institute in Pune, India, show that it is the same as a published sample with a different name that was collected from an abandoned mineshaft in southern Yunnan in 2013, following an outbreak of pneumonia-like illness that killed three miners there the year before. But that virus cannot be the immediate source of Covid-19. Part of one of its key genes, coding for the “spike” protein that allows the virus to lock onto human cells, is distinct from the version that is causing the pandemic. In the human virus, this part of the gene, called the “receptor binding motif,” more closely resembles the virus found in smuggled pangolins, though the rest of the pangolin virus is less similar. Compared with the bat and pangolin viruses, the one now infecting human beings also has an extra 12-letter nucleotide sequence, called a “furin cleavage site,” in the spike protein gene; this greatly enhances the virus’s ability to get into and out of different types of human cells. Kristian Andersen of the Scripps Institute in La Jolla, Calif., and colleagues argue that this might have arisen by mutation during “a period of unrecognized transmission in humans” after the original transmission from an animal.
...
So what did happen? At present, the evidence is pointing tentatively to a chain of person-to-person infections occurring somewhere outside a city before somebody brought the virus to Wuhan, where the market acted as an amplifier. The first case could have been a rural farmer or possibly a bat researcher collecting samples for virologists. Or it is possible that another animal was involved in some way, with the virus bouncing between a farmer and his animals, or a wildlife smuggler and his poor pangolins.
...
So what did happen? At present, the evidence is pointing tentatively to a chain of person-to-person infections occurring somewhere outside a city before somebody brought the virus to Wuhan, where the market acted as an amplifier. The first case could have been a rural farmer or possibly a bat researcher collecting samples for virologists. Or it is possible that another animal was involved in some way, with the virus bouncing between a farmer and his animals, or a wildlife smuggler and his poor pangolins.
May 30, 2020, 8:34 pm
#5374
Join Date: Aug 2014
Location: 42.1% in PDX , 49.9% in PVG & 8% in the air somewhere
Programs: Marriott Ambassador Elite, UA 1K, AS MVP GLD 75K, DL Pt
Posts: 1,086
2) The timeline for genetic evolution suggests a window from October - December --> The virus was mutating quietly before getting the features it needed for the highly contagious version we have.
3) Core of virus is closet to bat, the spikes are closely related to those from pangolins, but the core is NOT.
4) The current virus has another sequence very different from both the bat and pangolin
Model that there was a long chain of person to person outside of the city where the virus mutated to the current highly effective structure making it so suited for infections human-human. Then it was finally brought to Wuhan and the crowded market where that mutated / effective version soon became the Pandemic.
May 31, 2020, 7:41 am
#5375
Ambassador: Emirates Airlines
Join Date: Sep 2004
Location: Manchester, UK
Posts: 18,617
This is frightening...
 May 31, 2020, 5:27 pm
May 31, 2020, 5:27 pm
#5376
FlyerTalk Evangelist
Join Date: Jun 2005
Posts: 38,410
Jun 1, 2020, 8:52 am
#5377
Join Date: Mar 2005
Programs: Continental Onepass, Hilton, Marriott, USAir and now UA
Posts: 6,440
More data on efficacy of Remdesivir. From a Gilead press release
June 01, 2020
Gilead Announces Results From Phase 3 Trial of Remdesivir in Patients With Moderate COVID-19
" The study demonstrated that patients in the 5-day remdesivir treatment group were 65 percent more likely to have clinical improvement at Day 11 compared with those in the standard of care group (OR 1.65 [95% CI 1.09-2.48]; p=0.017). The odds of improvement in clinical status with the 10-day treatment course of remdesivir versus standard of care were also favorable, trending toward but not reaching statistical significance (OR 1.31 [95% CI 0.88-1.95]; p=0.18). No new safety signals were identified with remdesivir across either treatment group. Gilead plans to submit the full data for publication in a peer-reviewed journal in the coming weeks."
Hopefully, by Fall, we should have several treatments for the illness itself, even without a vaccine.
June 01, 2020
Gilead Announces Results From Phase 3 Trial of Remdesivir in Patients With Moderate COVID-19
" The study demonstrated that patients in the 5-day remdesivir treatment group were 65 percent more likely to have clinical improvement at Day 11 compared with those in the standard of care group (OR 1.65 [95% CI 1.09-2.48]; p=0.017). The odds of improvement in clinical status with the 10-day treatment course of remdesivir versus standard of care were also favorable, trending toward but not reaching statistical significance (OR 1.31 [95% CI 0.88-1.95]; p=0.18). No new safety signals were identified with remdesivir across either treatment group. Gilead plans to submit the full data for publication in a peer-reviewed journal in the coming weeks."
Hopefully, by Fall, we should have several treatments for the illness itself, even without a vaccine.
Jun 1, 2020, 9:04 am
#5378
Join Date: Dec 2018
Location: PHX
Programs: Delta DM, Marriott Lifetime Titanium, HHonrs Diamond
Posts: 1,336
Convalescent serum works well, but is limited by supply: https://www.cbsnews.com/news/coronav...es-2020-05-31/
Also, graph of survival rates...
Also, graph of survival rates...
Jun 1, 2020, 11:19 pm
#5379
A FlyerTalk Posting Legend
Join Date: Aug 2002
Location: NY Metro Area
Programs: AA 2MM Yay!, UA MM, Costco General Member
Posts: 49,040
Convalescent serum works well, but is limited by supply: https://www.cbsnews.com/news/coronav...es-2020-05-31/
Also, graph of survival rates...
https://twitter.com/EricTopol/status...92481072160771
Also, graph of survival rates...
https://twitter.com/EricTopol/status...92481072160771
Jun 2, 2020, 3:01 am
#5380


Join Date: Nov 2012
Location: Rhineland-Palatinate
Programs: *A Gold (A3), HHonor Gold
Posts: 5,699
A peer-reviewed statistical study from the RHEUM-COVID registry was published this week-end:
https://ard.bmj.com/content/early/20...is-2020-217871
Rather good news for people under biological therapy.
https://ard.bmj.com/content/early/20...is-2020-217871
Results: A total of 600 cases from 40 countries were included. Nearly half of the cases were hospitalised (277, 46%) and 55 (9%) died. In multivariable-adjusted models, prednisone dose ≥10 mg/day was associated with higher odds of hospitalisation (OR 2.05, 95% CI 1.06 to 3.96). Use of conventional disease-modifying antirheumatic drug (DMARD) alone or in combination with biologics/Janus Kinase inhibitors was not associated with hospitalisation (OR 1.23, 95% CI 0.70 to 2.17 and OR 0.74, 95% CI 0.37 to 1.46, respectively). Non-steroidal anti-inflammatory drug (NSAID) use was not associated with hospitalisation status (OR 0.64, 95% CI 0.39 to 1.06). Tumour necrosis factor inhibitor (anti-TNF) use was associated with a reduced odds of hospitalisation (OR 0.40, 95% CI 0.19 to 0.81), while no association with antimalarial use (OR 0.94, 95% CI 0.57 to 1.57) was observed.
Jun 2, 2020, 6:09 am
#5381
Join Date: Mar 2011
Location: BDL, JFK
Posts: 658
A peer-reviewed statistical study from the RHEUM-COVID registry was published this week-end:
https://ard.bmj.com/content/early/20...is-2020-217871
Rather good news for people under biological therapy.
https://ard.bmj.com/content/early/20...is-2020-217871
Rather good news for people under biological therapy.
Jun 2, 2020, 8:29 pm
#5382
Suspended
Join Date: Oct 2004
Location: Bay Area
Programs: DL SM, UA MP.
Posts: 12,729
Preprint of famotidine study available. Derek Lowe summarizes:
https://blogs.sciencemag.org/pipelin...he-coronavirus
So no action on slowing or stopping viral replication as hoped. But it may suppress histamine release, which may account for the runaway immune response with the inflammation of the lungs, cytokine storms. Or prevent mast cell granules release, which can be associated with loss of smell and taste.
The actual preprint is here.
https://www.researchsquare.com/article/rs-30934/v1
They also talk about the case of a 47-year old hospital worker who complained of fever, feeling of chess pressure, cough, shortness of breath and other symptoms. He took famotidine for 30 days. On other occasions when his SpO2 was low, he was put on a canal to raise oxygen levels. But gradually his symptoms improved and by days 27 and 28 he tested negative on PCR tests for the virus. Returned to work at day 31 and by day 47 he considered himself "largely recovered" though "he continues to note a lack of ability to taste or smell."
The takeaway from the study is that there needs to be more investigation of whether "dysfunctional mast cell degranulation" partially drives C19, specifically investigate whether other drugs for mast-cell disorders could reduce the severity and deaths of C19:
Then study whether such mast-cell disorder drugs could be combined with drugs which directly inhibit corona virus infection or replication to develop a safe and effective outpatient treatment before C19 vaccines become available.
As this new work details, an initial hypothesis was that the compound had some effect on one of the viral proteases, and you can still find that rationale if you start looking around for comments on the drug’s MOA. That hasn’t held up, though – the compound does not seem to be an inhibitor of these enzymes. Moreover, it is not effective in a cell-based infection model with the virus, either – basically, it’s not an antiviral in any sense of the term.
What does that leave you with? The downstream effects of being infected – all the cytokine storm stuff, the inappropriate immune response that gets so many patients into trouble. And that brings the histamine receptor mechanism back around again. The paper confirms that famotidine is a much more potent H2 ligand than is cimetidine (technically, it’s more of an inverse agonist than a classic antagonist), and moreover it seems to have different consequences on receptor binding. It seems to stimulate beta-arrestin binding to the receptor and subsequent internalization (a mechanism that complicates all sorts of G-protein coupled receptor signaling), and it appears that cimetidine doesn’t do this, either. There is also a possibility that the compound acts on the CCR2L and CXCR3 chemokine receptors, which would certainly be of interest, but this needs to be firmed up.
But one of the biggest differences between famotidine and cimetidine is in their pharmacokinetics. As the preprint illustrates, the higher potency and better blood levels of famotidine mean that it has much stronger coverage of the H2 mechanism in general, especially at the dosages that seem to have an effect in coronavirus infections. So here’s the paper’s mechanistic summary:
That’s an interesting and plausible idea – mast cells are what are involved in sudden histamine release – they’re sitting there loaded up with granules of the stuff, which can be dumped out on short notice. That’s an important part of a sudden anaphylaxis reaction, and mast cells are also involved in other immune response pathways, tissue permeability, and other processes. It’s certainly possible that they could be part of the inappropriate response to coronavirus infection and that inhibiting histamine release could be beneficial. The paper goes into details about lung physiology that tie the receptor’s action to some of the pathology seen in patients – for example, one thing that’s been noted is a lack of neutrophils and eosinophils in lung tissue samples, and both of these cell types have their activities inhibited by histamine release. In addition, the edema seen in coronavirus-affected lung tissue is unusual by the standards of viral infection, but makes more sense in light of a histamine-driven response. Mast cell degranulation also matches up with some of the other well-known symptoms (effects on smell and taste sensation, etc.)
The authors advance the idea, then, that many of the unusual features of the current virus in the clinic can be tied to histaminergic effects, and finish up this way:
What does that leave you with? The downstream effects of being infected – all the cytokine storm stuff, the inappropriate immune response that gets so many patients into trouble. And that brings the histamine receptor mechanism back around again. The paper confirms that famotidine is a much more potent H2 ligand than is cimetidine (technically, it’s more of an inverse agonist than a classic antagonist), and moreover it seems to have different consequences on receptor binding. It seems to stimulate beta-arrestin binding to the receptor and subsequent internalization (a mechanism that complicates all sorts of G-protein coupled receptor signaling), and it appears that cimetidine doesn’t do this, either. There is also a possibility that the compound acts on the CCR2L and CXCR3 chemokine receptors, which would certainly be of interest, but this needs to be firmed up.
But one of the biggest differences between famotidine and cimetidine is in their pharmacokinetics. As the preprint illustrates, the higher potency and better blood levels of famotidine mean that it has much stronger coverage of the H2 mechanism in general, especially at the dosages that seem to have an effect in coronavirus infections. So here’s the paper’s mechanistic summary:
The most straightforward explanation of the apparent famotidine activity as a COVID-19 therapy is that the drug acts via its antagonism or inverse-agonism of histamine signaling and via its arrestin biased activation—all a result of its binding to H2. If true, then it is reasonable to infer that a SARS-CoV-2 infection that results in COVID-19 is at least partially mediated by pathologic histamine release.
The authors advance the idea, then, that many of the unusual features of the current virus in the clinic can be tied to histaminergic effects, and finish up this way:
If COVID-19 is partially driven by dysfunctional mast cell degranulation, then a variety of medical interventions employing marketed drugs useful for treating mast cell-related disorders may help to reduce death and disease associated with SARS-CoV-2 infection. Examples include drugs with mast cell stabilizing activity, other histamine antagonists (for example H1 and H4 types), leukotriene antagonists and leukotriene receptor antagonists, anti-inflammatory agents such as those developed for inflammatory bowel diseases, and mast cell activation inhibitors. If such repurposed drugs are used in combination with pharmaceuticals that directly inhibit SARS-CoV-2 infection or replication, it may be possible to rapidly develop potent, safe and effective outpatient treatments for preventing or treating COVID-19 until such time as a safe and effective SARS-CoV-2 vaccine becomes available.
So no action on slowing or stopping viral replication as hoped. But it may suppress histamine release, which may account for the runaway immune response with the inflammation of the lungs, cytokine storms. Or prevent mast cell granules release, which can be associated with loss of smell and taste.
The actual preprint is here.
https://www.researchsquare.com/article/rs-30934/v1
They also talk about the case of a 47-year old hospital worker who complained of fever, feeling of chess pressure, cough, shortness of breath and other symptoms. He took famotidine for 30 days. On other occasions when his SpO2 was low, he was put on a canal to raise oxygen levels. But gradually his symptoms improved and by days 27 and 28 he tested negative on PCR tests for the virus. Returned to work at day 31 and by day 47 he considered himself "largely recovered" though "he continues to note a lack of ability to taste or smell."
Use of famotidine in this patient was recommended due to meeting FDA criteria for severe COVID-19 and his COVID-19 risk factors: male, 47yo, hypertension, obesity and diabetes mellitus Type 2. Although this is an anecdotal example, the patient experienced relief of symptoms overnight upon initiating use of famotidine. While not sufficient to demonstrate proof of cause and effect, this case does provide context for typical COVID-19 presentation and symptoms, as well as support for additional well-controlled famotidine therapeutic clinical trials in an outpatient setting.
The takeaway from the study is that there needs to be more investigation of whether "dysfunctional mast cell degranulation" partially drives C19, specifically investigate whether other drugs for mast-cell disorders could reduce the severity and deaths of C19:
other histamine antagonists (for example H1 and H4 types), leukotriene antagonists and leukotriene receptor antagonists 98, anti-inflammatory agents such as those developed for inflammatory bowel diseases, and mast cell activation inhibitors 99.
Jun 2, 2020, 8:40 pm
#5383
Suspended
Join Date: Oct 2004
Location: Bay Area
Programs: DL SM, UA MP.
Posts: 12,729
Recent survey of repurposed drugs being studied as possible treatments, their status.
https://www.nature.com/articles/d41591-020-00019-9
Among them, here is a pair that I haven't heard of elsewhere:
https://www.nature.com/articles/d41591-020-00019-9
Among them, here is a pair that I haven't heard of elsewhere:
Nafamostat and camostat are serine protease inhibitors both approved in Japan for use against pancreatitis in humans. Camostat was previously found in vitro to block the entry of SARS-CoV by acting as an antagonist to the serine protease TMPRSS2, and researchers believe both nafamostat and camostat could have a similar effect in inhibiting SARS-CoV-2. In vitro, both have been found to block the entry of SARS-CoV-2 into cells, although one preprint study reported that nafamostat inhibited viral cell entry with an efficiency roughly 15-fold higher than that of camostat.
These drugs are undergoing phase 2 and phase 2/3 clinical trials in the USA and Japan for their effectiveness against COVID-19, the primary outcome of which will be time to clinical improvement for nafamostat and reduced viral load after treatment for camostat.
“These drugs are quite old, they’re well studied, they have known targets that are exactly the same protease that the virus uses,” says Anton Yuryev, professional services director at Elsevier, who has done screenings for possible COVID-19 drug treatments.
These drugs are undergoing phase 2 and phase 2/3 clinical trials in the USA and Japan for their effectiveness against COVID-19, the primary outcome of which will be time to clinical improvement for nafamostat and reduced viral load after treatment for camostat.
“These drugs are quite old, they’re well studied, they have known targets that are exactly the same protease that the virus uses,” says Anton Yuryev, professional services director at Elsevier, who has done screenings for possible COVID-19 drug treatments.
Jun 3, 2020, 9:25 am
#5384
Join Date: Dec 2018
Location: PHX
Programs: Delta DM, Marriott Lifetime Titanium, HHonrs Diamond
Posts: 1,336
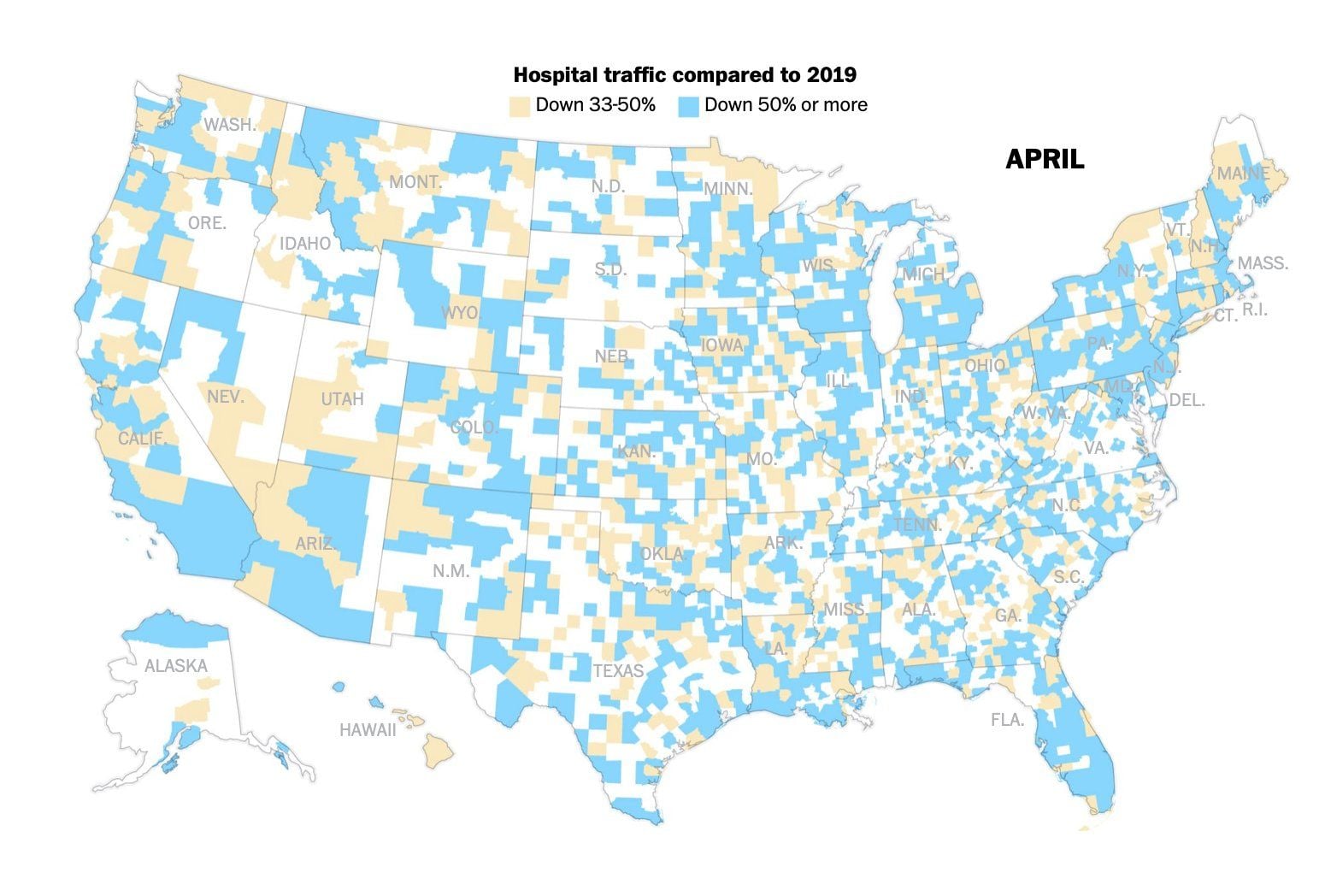
And now, the bigger health crisis as breast lumps and colon polyps continue to grow undiscovered and untreated...
From Washington Post, article behind paywall...
Note, even the white areas could be down, but less than 33%. Some of the white counties do not even have a hospital, which is the tragic reason why the county with the highest death rate in the USA (Early Co. Georgia) has 31 deaths but only 20 hospitalizations recorded.
From Washington Post, article behind paywall...
Note, even the white areas could be down, but less than 33%. Some of the white counties do not even have a hospital, which is the tragic reason why the county with the highest death rate in the USA (Early Co. Georgia) has 31 deaths but only 20 hospitalizations recorded.
Jun 3, 2020, 4:36 pm
#5385
Join Date: Oct 2007
Posts: 561
And now, the bigger health crisis as breast lumps and colon polyps continue to grow undiscovered and untreated...
From Washington Post, article behind paywall...
Note, even the white areas could be down, but less than 33%. Some of the white counties do not even have a hospital, which is the tragic reason why the county with the highest death rate in the USA (Early Co. Georgia) has 31 deaths but only 20 hospitalizations recorded.
From Washington Post, article behind paywall...
Note, even the white areas could be down, but less than 33%. Some of the white counties do not even have a hospital, which is the tragic reason why the county with the highest death rate in the USA (Early Co. Georgia) has 31 deaths but only 20 hospitalizations recorded.
I'm more concerned about the drop in stroke victims and heart attack patients. Those seem like a much larger increase in mortality and morbidity.