



















 Jan 27, 2020, 9:09 am
Jan 27, 2020, 9:09 am
Last edit by: username
PLEASE READ BEFORE POSTING
The following two links are updated daily:
IATA international transit / arrival policies Coronavirus Outbreak - Update
WHO Coronavirus disease (COVID-19) situation reports
Counters / Meters : Other Discussions on FlyerTalk Pertaining to COVID-19:
General (in this forum)
Location-specific
Airlines
Hotels
Other
Please add other discussions on FlyerTalk pertaining to COVID-19 not already been included in this WikiPost. Thank you.
This thread has become a valuable resource on Corona Virus/COVID-19 in general and no longer just about its impact on China travel. In order for the thread to remain fact-based and useful, posters are reminded to keep it free of speculation, conjecture and fear-mongering. Posts which do not meet these guidelines or which break the FT rules may be edited or deleted. Please observe the following FT rules in particular:
- be respectful and helpful
- stay on topic
- posts must be contributive to the thread
- inflammatory, inciting or unnecessarily provocative posts are not allowed
- repetitively posting comments of the same general theme is not permitted
- abusive, hateful, threatening, harassing or otherwise offensive posts will not be tolerated
- do not post comments on moderator decisions
FlyerTalk Senior Moderator Team
- be respectful and helpful
- stay on topic
- posts must be contributive to the thread
- inflammatory, inciting or unnecessarily provocative posts are not allowed
- repetitively posting comments of the same general theme is not permitted
- abusive, hateful, threatening, harassing or otherwise offensive posts will not be tolerated
- do not post comments on moderator decisions
FlyerTalk Senior Moderator Team
The following two links are updated daily:
IATA international transit / arrival policies Coronavirus Outbreak - Update
WHO Coronavirus disease (COVID-19) situation reports
Counters / Meters : Other Discussions on FlyerTalk Pertaining to COVID-19:
General (in this forum)
- Corona Virus / COVID-19 : general fact-based reporting [previously in] China forum
- COVID-19: Lounge thread for thoughts, concerns and questions
- USA halts entry of visitors who�ve been in UK, Ireland, Schengen countries
Location-specific
Airlines
- coronavirus travel waiver Air Canada | Aeroplan forum
- Coronavirus - Air China offers full refunds Other Asian, Australian, and South Pacific Airlines
- Does AFKL suspend flights to Mainland China? Air France, KLM, and Other Partners | Flying Blue
- NZ Suspends PVG service - till 29 March Air New Zealand | Air Points
- Alaska disappointing handling over an award ticket regarding viral outbreak in china Alaska Airlines | Mileage Plan
- AA China Coronavirus paid & award flights cancellation / change questions American Airlines | AAdvantage
- Coronavirus + NH All Nippon Airways | ANA Mileage Club
- *Coronavirus : BA Suspends all flts to mainland China* +discussion on long haul flts British Airways | Executive Club forum
- Wuhan coronavirus - effect on Cathay Pacific Cathay Pacific | Marco Polo Club
- China Southern travel-waiver corona-virus Other Asian, Australian, and South Pacific Airlines
- DL Coronavirus Waiver // Suspension of China flights due to Corona Virus Delta Air Lines / SkyMiles
- Coronavirus - Emirates Emirates | Skywards
- BR Adjusts Service/Schedule Due to Coronavirus Outbreak Eva Air / Infinity MileageLands
- Finnair China travel waivers?? Finnair | Finnair Plus
- Hainan Airlines (HU) Travel Waiver for 2019-nCoV? Other Asian, Australian, and South Pacific Airlines
- IB halts flights to China due to CoronaVirus [29/01/2020] Iberia Airlines | Iberia Plus
- Wuhan Coronavirus travel waiver / service change Japan Airlines | JAL Mileage Bank
- Coronavirus: LH Group general waiver to rebook flights operated end of April 2020 Lufthansa, Austrian, Swiss, Brussels, LOT and Other Partners | Miles & More
- Coronavirus: LH Group suspends flights to Italy [Discussion of Italy waiver] Lufthansa, Austrian, Swiss, Brussels, LOT and Other Partners | Miles & More
- Coronavirus Ticket Change Policy? Malaysia Airlines | Enrich
- QANTAS suspends services to China from Feb 9 Qantas | Frequent Flyer
- Ryanair - any options for Italy flights? Ryanair / Other European airlines
- SAS stops all direct flights to mainland China SAS | EuroBonus
- Coronavirus waivers Singapore Airlines | KrisFlyer
- THAI reduces flights to/from Mainland China 08Feb - 28Mar Thai Airways | Royal Orchid Plus
- Turkish Airlines Suspends Service to China until February 09 Turkish Airlines | Miles&Smiles
- UA COVID19: Flight Suspensions; Reduced serviced; Waivers; and No change fee bookings United Airlines | MileagePlus
- Coronavirus Waivers? Virgin Atlantic Airways | Flying Club
Hotels
- Cancellation of Bookings Due to Corona Virus Accor / ALL (Accor Live Limitless)
- Does Hilton wave no refundable bookings? Hilton / Hilton Honors
- CoronaVirus Cancellation - Non Refundable RESULT InterContinental Hotels / IHG Reward Club & Intercontinental Ambassador
- Coronavirus, any impact on your travel plan Marriott / Marriott Bonvoy
Other
- Which longhaul routes to/from China will be cut by end of Q1 2020? TravelBuzz
- Coronavirus epidemic, worries for China/ Global GDP OmniPR forum
- Coronavirus in the US. What would Amtrak do? Amtrak / Guest Rewards
- Your Next Cruise: Are are Having Second Thoughts Due to Fears of Pandemic? Travel&Dining / Cruises
Please add other discussions on FlyerTalk pertaining to COVID-19 not already been included in this WikiPost. Thank you.

Coronavirus / COVID-19 : general fact-based reporting
Feb 19, 2020, 10:48 am
#2176
Join Date: Oct 2007
Location: Southeast USA
Programs: various
Posts: 6,710
@trublu: Do you have any thoughts on the ACE-2 enzyme theory, that populations (such as Japanese and Han Chinese) who have higher levels of this in their lung tissues, are more susceptible to severe illness from COVID-19 than populations that have less of this enzyme?
 Feb 19, 2020, 10:51 am
Feb 19, 2020, 10:51 am
#2177
Suspended
Join Date: Oct 2004
Location: Bay Area
Programs: DL SM, UA MP.
Posts: 12,729
So far. Don't forget that people who became ill earlier are more likely to have already died (or recovered), while the outcomes for more recently diagnosed cases tend not to be known yet.
Part of the explanation for the worse outcomes on Wuhan/Hubei is surely the lack of adequate medical facilities and/or appropriate care. In addition, since this in an infectious disease, putting sick people together in crowded makeshift wards or hospital hallways to cross contaminate each other can't be helpful.
Part of the explanation for the worse outcomes on Wuhan/Hubei is surely the lack of adequate medical facilities and/or appropriate care. In addition, since this in an infectious disease, putting sick people together in crowded makeshift wards or hospital hallways to cross contaminate each other can't be helpful.
Is that even true though? If there's no cure, I'm not convinced "medical care" does anything at all to save a life. maybe prolong death, but has it been established that anyone that received medical care actually survived that otherwise wouldn't have?
To me it seems that even the best medical care (the doctor and the hospital's director come to mind) can't save anyone at all.
If you get it, it's up to your immune system and health to beat it. Medical care might make it [slightly] more comfortable, but that's about it.
To me it seems that even the best medical care (the doctor and the hospital's director come to mind) can't save anyone at all.
If you get it, it's up to your immune system and health to beat it. Medical care might make it [slightly] more comfortable, but that's about it.
My maxim is that one should avoid hospitals at all costs, until it becomes unavoidable. Hospitals are very dangerous places. But, if the alternative is likely death, being in hospital is just about a better option. I've repeatedly said (and not just on here) that the Chinese gov decision that mild cases should be institutionally treated is just insanity.
tb
tb
Would be interesting to know what proportion of those deaths are in hospital vs. at the deceased's home or somewhere else.
Maybe secondary infections are at play.
Also what would the treatment regime be, ventilators and retrovirals, maybe IV fluids and something to control fever?
Feb 19, 2020, 11:01 am
#2178
Join Date: Dec 2007
Location: PEK and BOS
Programs: BA - Blue
Posts: 4,531
@trublu: Do you have any thoughts on the ACE-2 enzyme theory, that populations (such as Japanese and Han Chinese) who have higher levels of this in their lung tissues, are more susceptible to severe illness from COVID-19 than populations that have less of this enzyme?
Going back to that preprint today, in the "comments" section someone has written a couple of days ago about an analysis they did on about 515 samples, most of them Caucasian and 8 Asians, but using a different methodology: "the result of comparison is shown below and in the figure; in my analysis I did not see significant difference between Asians and Caucasian in the ACE2 expression levels (P by two-tailed t-test = 0.858, P by generalized linear model [GLM] considering sex, age and type of death as covariates = 0.999). Also there was no difference between males (N = 300) and females" ....so according to this person, the Asian story doesn't add up, but they really need to publish their own data properly first.
tb
Feb 19, 2020, 11:06 am
#2179
Join Date: Dec 2016
Programs: BA Gold
Posts: 487
That's the approach they did use on the DP, but since so many people are asymptomatic, it's not really that helpful. You should of course prioritise testing/ isolation of symptomatic individuals, but mostly to identify those with severe illness, to offer early supportive therapy. If you think symptomatic screening will identify cases, the DP (and the German Wuhan evacuees) shows that's not going to work.
Err, not true. Many people in severe disease need 'supportive care, which may be as simple as a smidge of oxygen, Without this support, your body will tend to spiral round the drain, but with support, it allows host immunity to eventually kick in (or not) and alter outcomes. Now, I can't say how outcomes would be altered without supportive care: it's pretty unethical to not give oxygen to someone who needs it, so those sorts of trials aren't really possible. But the majority of severe/non-critical survive, and the severe category are people who would be receiving things like oxygen or intra-venous fluid support. We know from other infections that these supportive measures do make a huge difference to outcomes, and I would suggest the same is true here.
tb
tb
Feb 19, 2020, 11:16 am
#2180
Join Date: Dec 2007
Location: PEK and BOS
Programs: BA - Blue
Posts: 4,531
Exactly - it's all about buying time. Oxygen/bronchodilators/fluids/inotropes etc may not be disease modifying but they buy time for innate immunity to continue and adapative immunity (which can take several weeks) to begin. I think research now needs to focus on risk prediction - i.e. what are the risk factors which predispose to worse outcomes so that we can ensure people who are at high predicted risk have early access to good quality medical/intensive care and that healthcare systems are prepared with the right infrastructure for their populations.
tb
Feb 19, 2020, 11:29 am
#2181
Join Date: Feb 2013
Programs: Hyatt Globalist, MLife Gold, Marriott Gold, HHonors Gold, Caesars Diamond, Amex Plat
Posts: 5,948
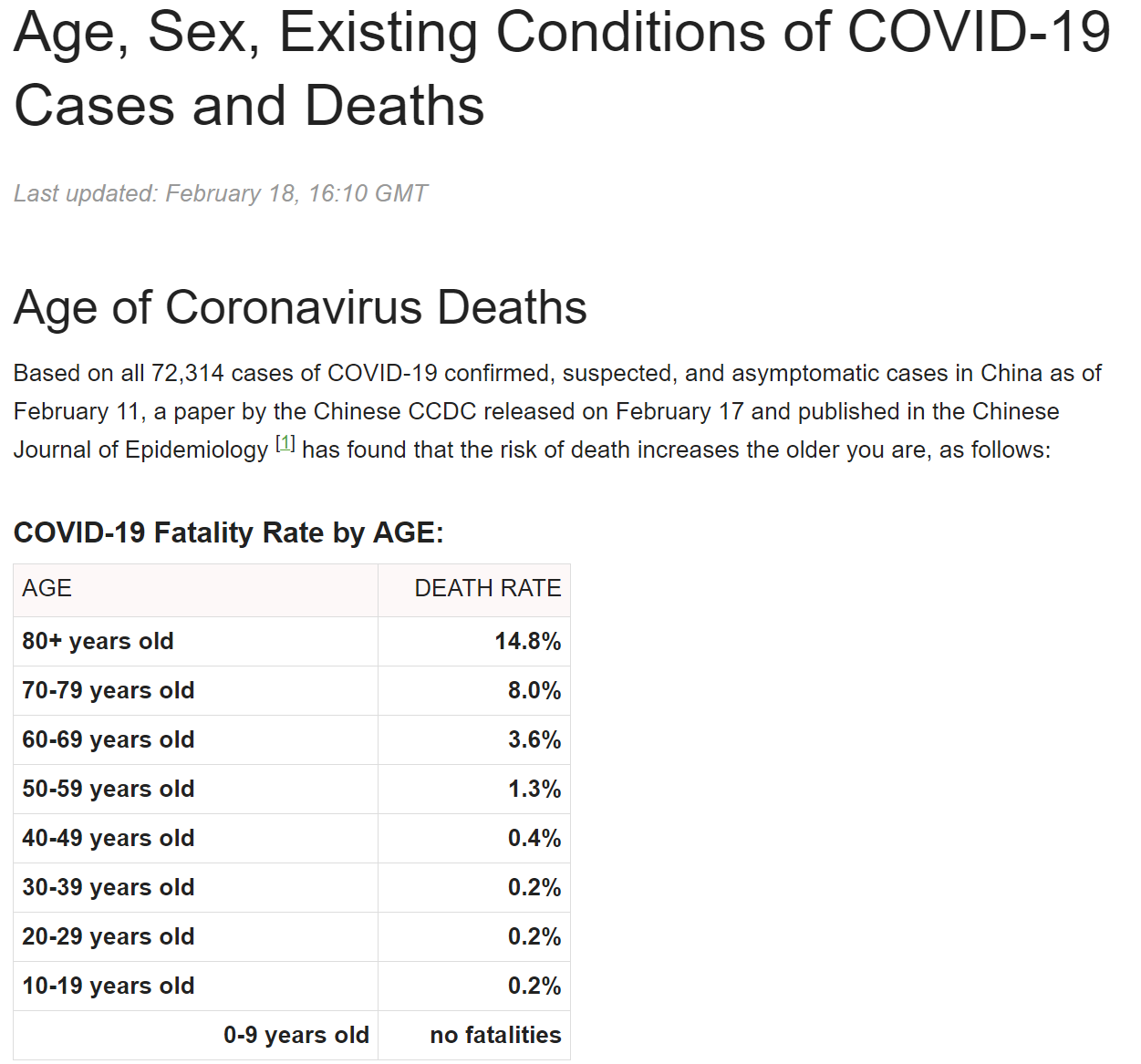
Is there any data re the ages (and perhaps exacerbating conditions) of patients who�ve died? The high profile deaths like the medic and hospital chief in Wuhan suggest that even those 30-55 are at serious risk.
Feb 19, 2020, 11:44 am
#2182
FlyerTalk Evangelist
Join Date: Nov 2004
Location: 45� North
Programs: DL DM MM, HH Diamond
Posts: 10,196
The number of deaths among those infected, known as the fatality rate, remains low but rises among those over 80 years old
https://www.bbc.com/news/world-asia-china-51540981
There is a chart in that article as well that shows fatalities by age group.
Feb 19, 2020, 11:55 am
#2183
Join Date: May 2013
Posts: 916
Can you get 2 versions of Flu at the same time ?
Say you have an average case of the yearly flu , you are weak but can still walk and do daily things ,
Can you also get Covid-19 since you are already weak ?
And since this is Winter in Wuhan could that be why its killed so many ?
Say you have an average case of the yearly flu , you are weak but can still walk and do daily things ,
Can you also get Covid-19 since you are already weak ?
And since this is Winter in Wuhan could that be why its killed so many ?
Feb 19, 2020, 12:00 pm
#2184
A FlyerTalk Posting Legend
Join Date: Sep 2009
Location: Minneapolis: DL DM charter 2.3MM
Programs: A3*Gold, SPG Plat, HyattDiamond, MarriottPP, LHW exAccess, ICI, Raffles Amb, NW PE MM, TWA Gold MM
Posts: 100,417
A more macabre place where we may end up if this all goes very badly wrong is to have two risk models: a) in the early stage of a pandemic, predictors of risk for very severe disease, and offer optimal supportive care. But once (and if) infrastructure starts to get overwhelmed, we may have to offer risk models of futility vs. likely recovery, and only offer supportive therapy to the latter. An absolutely horrid place to be, but something that's routinely done outside of the US.
tb
tb
OTOH, when we discuss testing and screening, for example on the Wuhan Princess or in the Wuhan area, what's the goal? The goal of quarantine, to be brutal, is to protect the rest of the population and not necessarily to protect or improve the health of those being quarantined, although of course it would be unethical to just lock them up and wait to see who dies. Ideally, we'd like to protect the people being quarantined, including especially those who have not yet caught the disease (although unless it can be spread before symptoms appear, there's no reason to quarantine anyone who is certainly asymptomatic). For the Wuhan Princess, one strategy might have been to remove anyone showing symptoms (essentially giving them a presumptive diagnosis of WuFlu without any testing), isolate and treat the same as ordinary flu, perhaps testing if more aggressive treatment appears necessary. Then save the scarce testing capacity for asymptomatic individuals, perhaps giving priority to crew distributing meals or to passengers sharing rooms with multiple other occupants.
IMO much of the failure stems from lack of a clearly articulated goal and associated plan, combined of course with the face saving determination to release passengers after fourteen days regardless of any evidence about the spread of WuFlu. Another part of the problem seems to be that appropriate expertise wasn't consulted to help with decision making, including decisions about procedures to be followed by crew and lower level medical workers.
Feb 19, 2020, 12:00 pm
#2185
Ambassador: China
Join Date: Oct 2005
Location: Malibu Inferno Ground Zero
Programs: UA AA CO
Posts: 4,836
Improvised BioHazard suit.
Two Jetstar flight passengers in Australia wrapped themselves in plastic sheets amid fears of the coronavirus, viral footage shows.
https://nypost.com/2020/02/19/fliers...navirus-fears/
https://nypost.com/2020/02/19/fliers...navirus-fears/
Feb 19, 2020, 12:03 pm
#2186
FlyerTalk Evangelist
Join Date: Nov 2004
Location: 45� North
Programs: DL DM MM, HH Diamond
Posts: 10,196
Two Jetstar flight passengers in Australia wrapped themselves in plastic sheets amid fears of the coronavirus, viral footage shows.
https://nypost.com/2020/02/19/fliers...navirus-fears/
https://twitter.com/Alyss423/status/1229972896371462144
https://nypost.com/2020/02/19/fliers...navirus-fears/
https://twitter.com/Alyss423/status/1229972896371462144
Feb 19, 2020, 12:18 pm
#2187
Join Date: Dec 2007
Location: Virginia City Highlands
Programs: Nothing anymore after 20 years
Posts: 6,900
Here we go... new development
How did they die so quickly? Or were they sick before and no one thought to run tests on the virus on them?
Two Iranians die after testing positive for coronavirus: official
How did they die so quickly? Or were they sick before and no one thought to run tests on the virus on them?
Feb 19, 2020, 12:31 pm
#2188
Join Date: Dec 2007
Location: Virginia City Highlands
Programs: Nothing anymore after 20 years
Posts: 6,900
 Feb 19, 2020, 12:31 pm
Feb 19, 2020, 12:31 pm
#2189
FlyerTalk Evangelist
Join Date: Nov 2004
Location: 45� North
Programs: DL DM MM, HH Diamond
Posts: 10,196
Here we go... new development
How did they die so quickly? Or were they sick before and no one thought to run tests on the virus on them?
Two Iranians die after testing positive for coronavirus: official
How did they die so quickly? Or were they sick before and no one thought to run tests on the virus on them?
Feb 19, 2020, 12:39 pm
#2190
Join Date: May 2010
Location: AVP & PEK
Programs: UA 1K 1.9MM
Posts: 6,358
Thanks for that!
Still amazing that no kids died (same as for SARS).
Has there been more research into a possible connection to Measles/Rubella vaccinations and elevated immunity to COVID-19?